Moving from SMALED and CMT into DYNC1H1-Related Disorders
Navigating a rare genetic diagnosis is challenging, but it becomes exponentially more difficult when a condition has multiple names, highly variable symptoms, and overlaps with more famous neuromuscular diseases. This is the reality for individuals with DYNC1H1-Related Disorders (DRD). The DYNC1H1 Association has put together this guide in hopes of assisting patients and their care teams understand how DRD overlaps - sometimes - with each of these conditions.
Prior to the advent of modern genetic testing in the past decade, patients with DYNC1H1-related disorders would have been diagnosed with symptomatic disorders. Most notably SMA-LED (Spinal Muscular Atrophy with Lower Extremity Predominance), Charcot Marie Tooth Disease, or neurological and behavioral disorders, like cerebral palsy or idiopathic intellectual disability. As genetic sequencing has become more commonplace, experts now recognize these symptomatic disorders as components in the complex spectrum of symptoms linked with DYNC1H1-related conditions.
Because DRD is so rare, your multidisciplinary care team - including physicians, physical therapists (PTs), occupational therapists (OTs), speech-language pathologists (SLPs), behaviorists, and feeding specialists may not have encountered it before. They may look at a "SMALED" or "CMT" label on a chart and make assumptions based on classic presentations of those diseases, missing the unique needs of a DYNC1H1 patient.
This guide, built from peer-reviewed literature and resources like GeneReviews, serves as an educational tool to share with your clinicians. It outlines how DYNC1H1-related disorders compare to other classic conditions and highlights the some key care nuances your team needs to know.
The Root Problem: What is DYNC1H1?
To understand this condition, it helps to look inside the cell. The DYNC1H1 gene provides instructions for making a massive protein called cytoplasmic dynein heavy chain 1. Dynein’s job in the cell is to move materials around the cell by walking along cellular "highways" called microtubules.
Dynein is responsible for retrograde axonal transport—moving essential cellular machinery, proteins, and waste products from the far ends of a nerve cell (like the tips of your toes) back up to the main cell body. It is also deeply involved in how neurons migrate and find their proper places in the brain during fetal development.
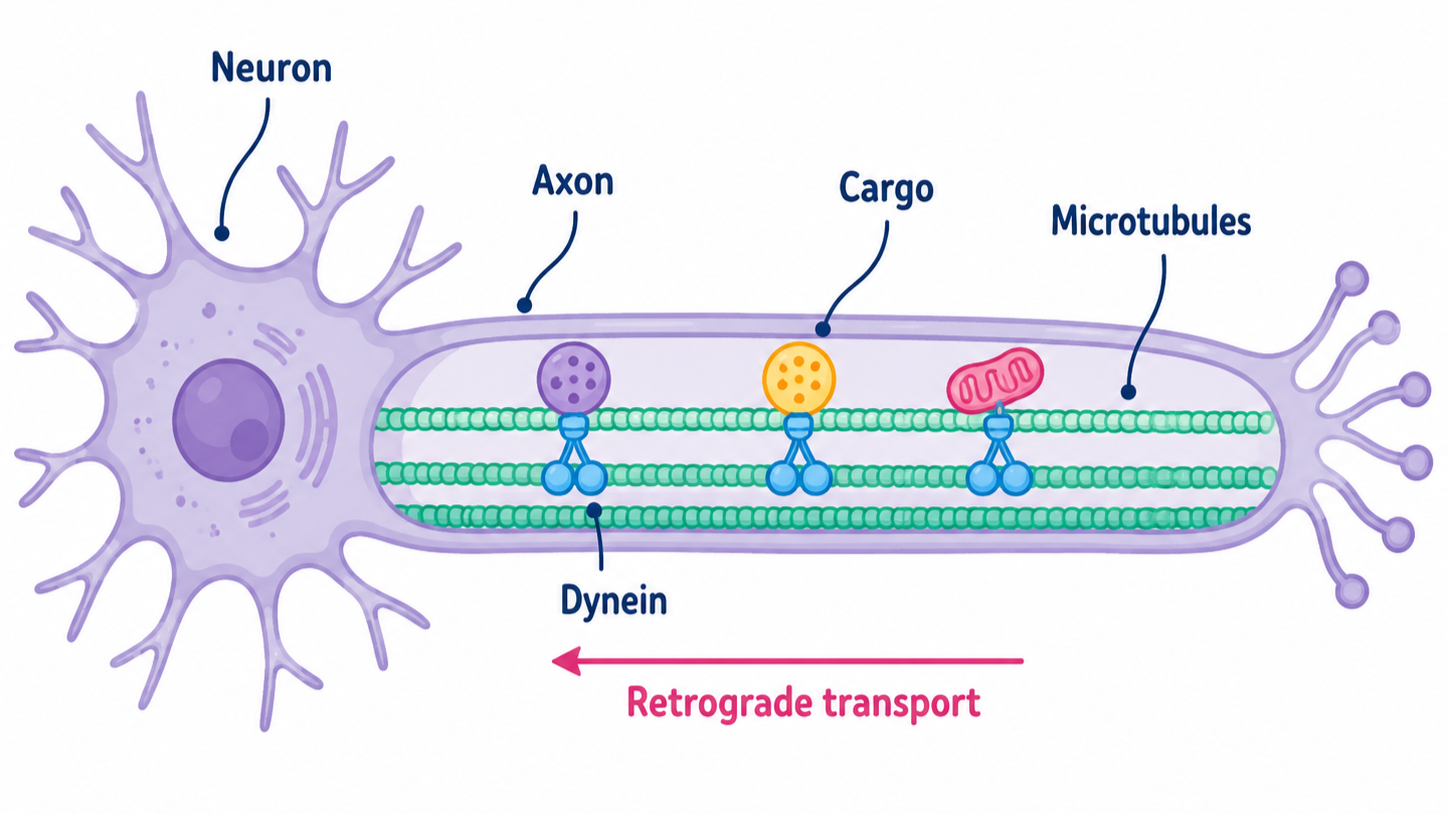
Dynein is responsible for carrying hundreds of different materials from the tip of a cell back towards its nucleus. Credit: Amish Bhatnagar, UC Berkeley 2026
When a mutation occurs in DYNC1H1, the "trucks" move in irregular fashions. Some stall or stutter, while some speed. No matter the impact, these gene variants in dynein cause issues with vital materials shipping (called trafficking) in the cells. Increasing distance or size of cargo can exacerbate these symptoms. Because motor nerves stretching down to the legs are the longest cells in the body, they often suffer the most from this transportation breakdown.
Facing the Challenge of Heterogeneity
The greatest hurdle in treating DYNC1H1-related disorders is their immense clinical heterogeneity (variability). Two people with mutations in the exact same gene can have vastly different lives. In the 2024 GeneReviews article, the author describes the clinical spectrum as generally split into two broad categories based on where the mutation falls on the gene. That said, the same author is in the process of updating the publication to specify that DRD fits the profile of a spectrum disorder, where any patient may have any combination of symptoms.
This means a DYNC1H1 patient might have normal cognition but severe walking difficulties, or they may have mild physical symptoms but complex behavioral and speech challenges, or any severity of symptoms overall. For more information on this, please see the DA’s Welcome Packet or our “Newly Diagnosed” page.

DRD is a highly variable disorder, with this graphic showing five possible symptom profiles. Credit: Amish Bhatnagar, UC Berkeley, 2026.
The Clinical Comparison Table
Clinicians are trained to recognize patterns. Because DYNC1H1 presentations mimic other diseases, sharing this comparative breakdown can help your providers understand how it aligns and diverges from classic neuromuscular diagnoses. This knowledge can help them make a more appropriate care plan for your loved one.
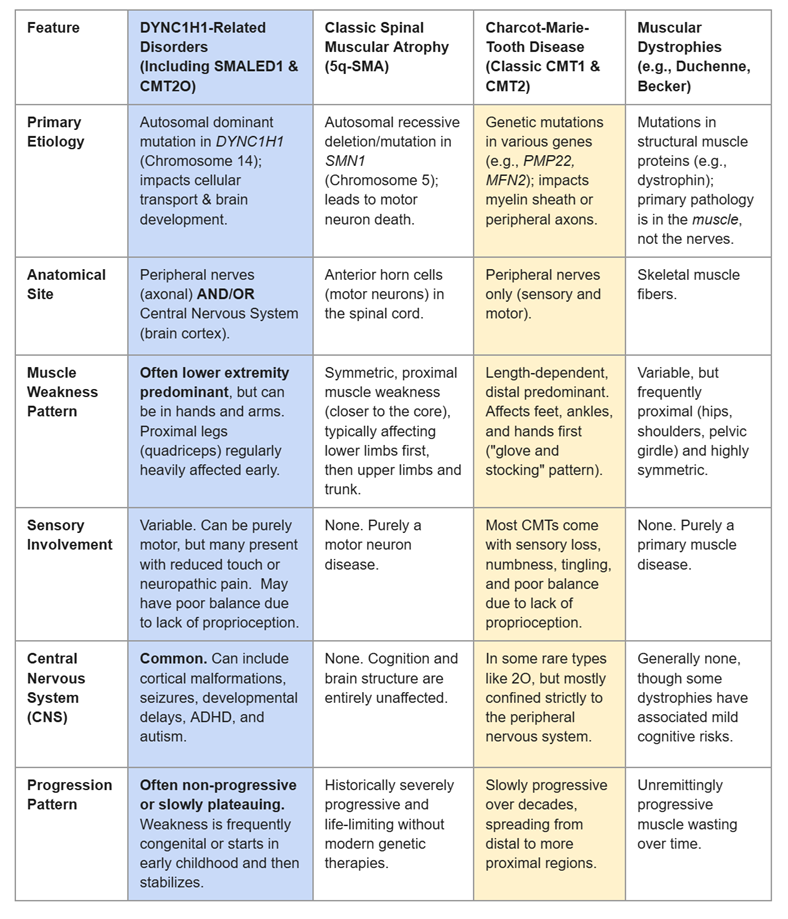
Table comparing common neuromuscular disorders that have symptomatic overlap with DRD.
Helpful Insights for Your Multi-Disciplinary Team
When sharing this with your providers, the following might be of greatest interest to them:
For Physical and Occupational Therapists (PT/OT)
The "Tricky" Proximal Weakness: Unlike classic CMT, which wastes the calves and ankles first, DYNC1H1 frequently mimics SMA by targeting the quadriceps and hips first. Patients often present with a waddling gait or a positive Gower’s sign (using hands to "walk" up the legs to stand). Bracing strategies must account for hip and knee instability, not just foot drop. In addition, this distal weakness can extend to the hands, making fine motor control difficult.
Expect a Plateau, Not Continuous Decline: Unlike muscular dystrophy, DYNC1H1 is often static or very slowly progressive after early childhood. PT goals should focus on maximizing function, preventing contractures, and managing orthopedic issues (like hip dysplasia or scoliosis), rather than preparing for rapid, unremitting decline. Exercise generally benefits patients with DRD, and intensive therapies have shown benefit for many patients.
The Sensory-Motor Disconnect: Do not assume a patient’s clumsy gait is entirely due to weakness. Axonal transport issues compromise proprioception (the brain's awareness of where limbs are in space). Balance training should heavily rely on visual cues and stable environments. Note that some patients may also have cortical visual impairment, reducing their ability to perceive the environment, so screening for visual impairments are key.
The Behavior-Motor Challenges: Many patients with DRD a challenged by their attention spans, sensory processing difficulties, and intellectual ability. In addition, some have tremors with tired muscles or myoclonic seizures that are out of their control. Developing strategies that enable access to strengthening therapies can often be the largest hurdle to a successful therapeutic program.
For Speech and Feeding Specialists (SLPs)
Early Bulbar and Feeding Challenges: According to patient registries like Simons Searchlight, infants with DYNC1H1 mutations frequently present with early hypotonia (low muscle tone), weak sucking, severe gastroesophageal reflux (GERD), or aspiration risks. Some patients may benefit from a G-tube. In addition, constipation is a common symptom that could impact appetite.
Central vs. Peripheral Causes: If a child has feeding or speech delays, it may be a combination of low muscle tone and central processing deficits (due to cortical brain malformations). Autonomic dysfunction is seen in patients, leading to difficulties with interoception. One family reports that their daughter didn’t connect her stomach pain to hunger until she was over ten years old.
Augmentative Communication: For individuals on the severe end of speech apraxia or lack verbal language, early introduction of Augmentative and Alternative Communication (AAC) methods—such as switches, pictograms, or eye-gaze tech—is encouraged. As stated previously, this should be paired with a functional vision assessment.

Even verbal children with DRD may benefit from supports like AAC during feeding therapy to allow the patient complete focus on feeding. Credit: Amish Bhatnagar, UC Berkeley 2026.
Summary for Clinicians
The Takeaway: DYNC1H1-related disorder is a unique genetic entity. It is not "just" SMA because it can include structural brain changes, autism, and sensory neuropathies. It is not "classic" CMT because the weakness is primarily proximal (thighs/hips) rather than distal (feet/calves) and often plateaus. Even progression of DRD is different - patients may retain their strength and function until their 50s, or may go through sudden and dramatic reductions in function at a random point in their lives. Treatment plans must be highly customized, treating the specific physical and neurodevelopmental profile of the individual rather than the historic diagnostic umbrella.
Reliable Sources & Further Reading
GeneReviews®: DYNC1H1-Related Disorders (Birk Möller et al.) – Comprehensive medical overview of diagnostic criteria and clinical management.
Simons Searchlight: DYNC1H1 Gene Guide – Patient-centered data tracking the phenotypic spectrum and developmental impacts.
The DYNC1H1 Association: Official advocacy and research network mapping the cellular mechanics of dynein mutations, organizing patient communities, and driving research for a cure.
UNIQUE: DYNC1H1-Related Disorders Gene Guide - Comprehensive patient guide for families and clinicians looking to improve their understanding of DRD.